
🚀 Discover this trending post from Hacker News 📖
📂 **Category**:
📌 **What You’ll Learn**:
Health data
To explore the relationship between politics and health, we draw on the Add Health survey. Add Health is an ongoing survey tracking a nationally representative cohort in the USA, first interviewed while in grades 7–12 in 1994. So far, this cohort has been interviewed five times.
Add Health interviews include survey questions on demographic and health attributes and measurements of ‘biomarkers’ collected in survey takers’ homes by trained interviewers. Five biomarkers are measured in both waves 4 and 5, which are our focus here: body mass index, lipids (that is, cholesterol), HbA1c levels, blood pressure and C-reactive protein levels. Add Health has also checked respondents’ vital status against the National Death Index up to 2022 to determine whether respondents have died. Because of their age, mortality is a rare, although important, outcome in this sample: those interviewed in wave 5 were born between 1974 and 1983, with over 92% born between 1977 and 1982. By 2021–2022, the cohort was largely between 40 and 45 years old.
In the third (2001–2002), fourth (2008–2009) and fifth (2016–2018) survey waves, Add Health also asked respondents whether they identified as very liberal, liberal, moderate, conservative or very conservative. Although Add Health does not have a usable measure of party identification or vote choice, it is worth emphasizing that its inclusion of any questions about political orientation makes it unusual among health surveys.
Due to Add Health’s school-based sampling design, standard errors are clustered at the school level. All data are weighted to be representative of the cohort in the given wave.
Ideology and health markers during the lifetime
Figure 1 shows the average number of comorbidities (out of five measured biomarkers; see Methods for details) for liberals and conservatives, as measured in waves 4 and 5. Higher numbers represent more total comorbidities and thus poorer health (Supplementary Section 1 presents results by individual measure). In 2008–2009 (wave 4), no discernible relationship exists between biomarkers (taken in 2008–2009) and ideological identification (as expressed in the 2008–2009 survey). An equivalence test presented in Supplementary Table 4 suggests that there is no difference greater than 0.04 between the most liberal group and any other.
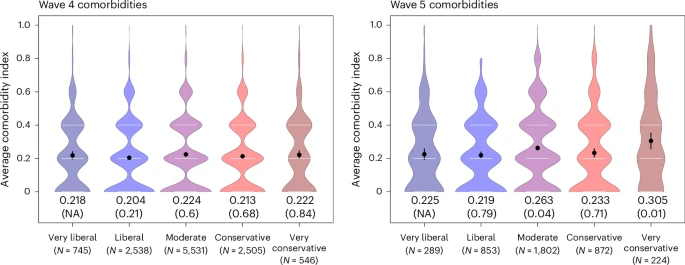
Health status by ideological self-identification in wave 4 (2008–2009) and wave 5 (2016–2018) of the Add Health survey. Both ideology and health are measured in wave 4 and wave 5; each represents contemporaneous health and ideological measures. Black points represent the average and black vertical lines are the 95% CI. The thin horizontal grey lines represent quartiles. Density is underlaid. The comorbidity index is a combined measure of the five health indicators for respondents with each measure. P values, in parentheses, are the difference between the category and those identified as very liberal using OLS regression, with two-sided test for significance. Full statistical reporting is provided in Supplementary Section 1.2. P value is not applicable (NA) for very liberal respondents.
However, by 2016–2018, the most conservative respondents (as measured in 2016–2018) were the least healthy (as measured in 2016–2018) (mean (M) = 0.305; 95% CI, (0.26, 0.36)). Table 1 shows the differences in the wave 4 and wave 5 cross-sections. The gap in health between the most liberal and conservative respondents in wave 5 represents one-third of the comorbidity scale’s standard deviation, making it statistically and substantively significant (0.08, 95% CI; (0.02, 0.14); P = 0.014). Supplementary Section 1.2 shows full tabular regression results.
What explains conservatives becoming less healthy than liberals between 2008 and 2016? The panel structure of the Add Health data allows us to separate two competing explanations: within-individual changes in health, where people who were already conservative in 2008 declined in health by 2016, or changes in ideology, where people who were less healthy in 2008 became more conservative by 2016.
Figure 2 shows health in waves 4 and 5 among respondents who maintained and changed their ideological beliefs over time. Each plot shows health among the same group of respondents in both waves. For simplicity and power, we group together very liberal and liberal (and very conservative and conservative) respondents; Supplementary Fig. 2 suggests this decision to group categories is not consequential for our substantive conclusions. Nearly every group became less healthy (that is, a higher comorbidity score) over time, as respondents aged between 2008 and 2016. But this change was not equal across groups: respondents who identified as liberals in wave 4 but ‘became conservative’ by wave 5 (Fig. 2, second plot) were slightly less healthy than other liberals in wave 4, but they became much less healthy than liberals (and indeed other conservatives) by wave 5. Meanwhile, people who became liberal between waves were healthier in wave 4 and became, if anything, more healthy by wave 5. This suggests that small differences in health in wave 4 predicted changes in ideology—and magnified differences in health—by wave 5.

Health in waves 4 and 5 among people who were liberal or conservative in wave 4 or 5, divided by their pattern of ideological change or stasis between waves (listed across the top of each plot). ‘Stayed conservative (liberal)’ respondents were conservative or very conservative (liberal) in both waves. ‘Became conservative (liberal)’ respondents were liberal or very liberal (conservative) in wave 4 and conservative or very conservative (liberal) in wave 5. ‘Moderate one wave’ respondents were moderates in either wave 4 or 5 and liberal or conservative in the other wave. Health is measured by a comorbidity index, a combined measure of the five health indicators for respondents with each measure, so higher levels indicate worse health. Means for each group wave are marked with an X; density is underlaid, with 25th, 50th and 75th percentiles marked with grey lines.
Supplementary Table 5 presents a similar analysis using a cross-lagged dependent variable, with wave 4 health predicting wave 5 ideology and wave 4 ideology predicting wave 5 health. Those who are less healthy in wave 4 became significantly more conservative between waves 4 and 5, although the relationship loses statistical significance once controlling for demographics. Wave 4 ideology does not predict changes in health by wave 5.
To understand the contribution of each group to the overall growth of the ideological gap, the left-hand plot in Fig. 3 decomposes the change along different dimensions. The overall gap in health between liberals and conservatives grew by 0.034 between waves. The left-hand plot in Fig. 3 shows that half of this change can be attributed to respondents who ‘flipped’ between liberal and conservative between waves (dark grey), while one-third is explained by subtler changes among the larger group of respondents who remained liberal or conservative in both waves (light grey). Only a small share is due to the respondents who shifted between moderate and either ideological fold (black).
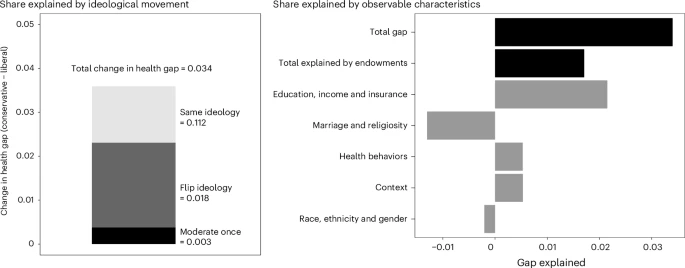
Left: Decomposition of the change in the gap in biomarkers between liberal and conservative respondents between wave 4 and wave 5 into the share of the gap attributable to three groups: ‘Same ideology’ (liberal or conservative in both waves), ‘flip ideology’ (liberal in one wave and conservative in the next, or vice versa) and ‘moderate once’ (liberal or conservative in one wave and moderate in the other). Right: the gap attributable to changes in the liberal and conservative groups’ ‘endowments’ of observable characteristics, followed by the gaps attributable to five categories of observable characteristics.
So why might less healthy people become more conservative in this era—and already conservative people become less healthy? To explore this, the right-hand plot in Fig. 3 next presents the results of a Kitagawa–Oaxaca–Blinder decomposition20, a method that describes what proportion of the change in the health gap between liberals and conservatives over time can be attributed to changes in their observable characteristics, including demographics, health behaviours, contextual factors and socio-economic status.
Half of the increase in the health gap between liberals and conservatives over time (0.017 of 0.034) can be attributed to changes in these observable characteristics of the groups. A share of this is due to liberals’ relative gains in socio-economic status, including education, income and access to health insurance, all of which are associated with better health. For example, liberals went from being slightly less likely to have health insurance in wave 4 to slightly more likely in wave 5. This aligns with recent work showing more educated—and thus typically healthier21—Americans have become more liberal in recent years22.
Liberals were also helped, on balance, by relative gains in their lifestyle factors (including more exercise and less consumption of sugary drinks) and living in healthier places. Conversely, the gap between liberals and conservatives would have grown more if not for conservatives’ relative gains on two health-promoting dimensions: marriage and religiosity. Race, ethnicity and gender play small roles.
The remaining half of the increase in the health gap is not explainable by these observable factors. It could be due to the gaps in measured characteristics such as education or health behaviours becoming more impactful on health over time. Or, in a more intrinsically political sense, it could be due to unmeasured differences between liberals and conservatives—such as their values, beliefs or relationships to medicine—drifting further apart.
Mortality over time
We next turn from measures of poor health during the lifetime to a downstream consequence: mortality. In addition to measuring biomarkers in wave 4 and wave 5, Add Health tracks each respondent’s vital status against the National Death Index, an index of deaths and their underlying cause administered by the US Centers for Disease Control and Prevention (CDC).
Figure 4 shows the relationship between vital status in a given 3-year period, starting in the year listed along the x axis, and ideological self-identification as measured in a given wave. The left-hand plot shows deaths of all causes, the middle plot shows internal causes of death (sometimes called disease-based deaths, such as those from heart disease or cancer), and the right-most plot shows deaths from an external cause (for example, car accidents or drug overdoses). Using a linear probability model, we regress mortality on ideology measured on a 5-point scale from very liberal (coded as 0) to very conservative (coded as 1); the coefficient can be interpreted as the change in the probability of death going from the most liberal end of the political spectrum to the most conservative (presented in percentage points out of 100). The blue lines in Fig. 4 represent probability of death in the 3-year bin on the x axis by ideological self-identification as measured in wave 3 (2001–2002), black lines in wave 4 (2008–2009) and red lines in wave 5 (2016–2018).
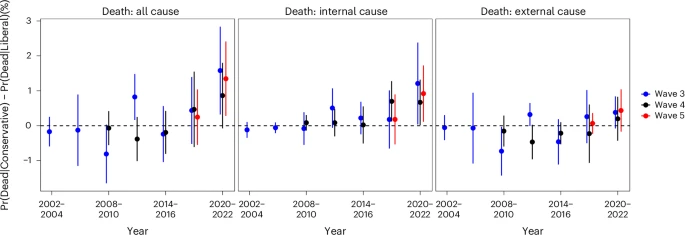
Each point is the difference in the predicted probability (Pr) of death in a given 3-year period between the most liberal and most conservative respondents. A binary indicator of death (0–1) is regressed on a 5-point ideological scale (rescaled from 0 to 1) (using OLS; to display as a percentage point change, we multiply by 100). Higher values represent higher mortality rates for conservatives. Lines represent 95% CIs (2-sided t-test); standard errors are clustered at the school level (sampling unit). For example, the right-most points (at 2020) show the relationship between ideological as measured in waves 3–5 for deaths between 2020 and 2022. Ideological identification ranges from very liberal (0) to very conservative (1) as measured in wave 3, wave 4 and wave 5. Supplementary Section 5 has full statistical results. A total of 12,962, 13,892 and 11,477 respondents answered the question on ideology (and had a corresponding cross-sectional weight) in wave 3, wave 4 and wave 5, respectively.
We use 3-year bins to illustrate change over time while ensuring enough power given the relatively few deaths in any given year. As the timing of the survey waves did not overlap perfectly with 3-year bins, the 2008–2010 points for wave 4 and 2017–2019 points for wave 5 only reflect data from respondents who completed the survey by that year (wave 4 was conducted in 2008–2009 and wave 5 in 2016–2018). Supplementary Section 4 presents results by year and cumulatively, and the main results using a logit rather than ordinary least squares (OLS) model.
The negative coefficients in the first years of all-cause deaths show that liberals died at rates higher than or similar to conservatives in the early 2000s, although the coefficients do not statistically differ from zero. However, by 2020–2022, more conservative respondents (as measured in waves 3 and 5) were significantly more likely to die than more liberal ones (wave 3, coefficient (β) = 1.58, 95% CI, (0.32, 2.83), P = 0.014; wave 5, β = 1.35, 95% CI, (0.28, 2.41), P = 0.014).
Decomposing deaths between external and internal causes shows what is driving this shift. Conservatives began to trail their liberal peers in internally caused death in the late 2010s, although only wave 4 measures show statistical significance before 2020 (in 2017–2019, β = 0.7, 95% CI, (0.12, 1.28), P = 0.018). In the final time period (2020–2022), conservatives died more often of internal causes such as cancer, heart disease and diabetes—that is, causes related to attributes measured in the biomarker data, such as blood pressure and cholesterol. The linkage between ideology and mortality is consistently significant only after 2020, a point we will return to in the next section (wave 3, β = 1.21, 95% CI, (0.04, 2.38), P = 0.043; wave 4, β = 0.67, 95% CI, (0.02, 1.32), P = 0.04; wave 5, β = 0.92, 95% CI, (0.11, 1.73), P = 0.026). This pattern—the growth of death on the right—is weak or absent in externally caused deaths.
One explanation for this trend is that ideology generally becomes more linked to health outcomes as people age, meaning a similar gap would appear over time among similarly aged cohorts in previous years. Older data on politics and mortality provide evidence against a pure age effect: cohorts born in the decades before the Add Health group did not experience a growing link between their ideology and vital status over their 30s and 40s (Supplementary Section 3).
Another possibility is that ideology became more linked to health outcomes during the 2010s for reasons specific to this cohort of people, but not for older or younger cohorts. Without more recent data on a broader age group, we cannot say whether the years 2005–2022 represented a period of change across cohorts. The potential explanation we offer for these changes in the section ‘Politics and health after COVID-19’, however, is not specific to this cohort.
Mortality in the COVID-19 era
Although ideology became more predictive of health during the 2010s, the relationship between politics and mortality became consistently significant only after 2020. This raises an important question: is the rise in conservatives’ mortality driven by, or even fully reducible to, the effects of COVID-19? Previous work23 has found that Republicans died of COVID-19 at higher rates than Democrats, especially after vaccine roll-out.
To test this, Table 2 investigates internally caused deaths in the final 3 years for which Add Health data are available: 2020, 2021 and 2022. Each model regresses mortality in 2020–2022 on political and demographic features of Add Health participants. Coefficients on each ideological subgroup represent the difference in mortality between people identifying as very liberal (the omitted category) and those in other groups, using a linear probability model. For reference, column 1 in Table 2 shows the predicted probability of internally caused death since 2020 as a function of ideological self-identification only. For these models, we use wave 5 ideology and demographics. Supplementary Section 7 presents results using various measures and weighting schemes.
A strong relationship appears: participants who identify as very conservative were about 1.144 percentage points (95% CI, (0.18, 2.11); P = 0.021) more likely to die in 2020–2022 than those who were very liberal. Unlike in the biomarker analyses, moderate, conservative and very conservative respondents showed worse health—not only the most conservative.
Columns 2 and 3 in Table 2 draw on granular cause-of-death data to divide deaths from COVID-19 (column 3) from deaths from all other internal causes (column 2). Even once COVID-19 deaths are separated out, column 2 shows that liberals, moderates and conservatives were all more likely to die during the 2020–2022 period than the most liberal respondents.
One possibility is that COVID-19 deaths are misclassified as non-COVID-19 deaths. It is not possible to entirely rule out this explanation. However, the low COVID-19 mortality rate as reported by the CDC among this age group casts doubt on this explanation. We also checked second- and third-order causes of death (rather than underlying cause of death) to see if COVID-19 was a secondary factor; it was not.
What else might explain conservatives’ higher death rates during this period? As in our analysis of biomarkers, we can test the extent to which the gap is explained by observable differences between liberals and conservatives, including their demographics, resources and geographic contexts. The remaining columns of Table 2 regress internally caused deaths on ideology and a range of covariates related to these explanations.
Column 4 in Table 2 shows that a range of individual-level characteristics fail to fully explain the gap between the most liberal and conservative respondents. While race, ethnicity and income predict mortality, the coefficients on ideological groups remain large and statistically significant.
Column 5 in Table 2 moves beyond individual characteristics to geographic context. Much of the previous work on the relationship between health and politics compares health outcomes between more-and-less conservative localities (for example, counties or states). Differences in mortality between liberals and conservatives in these analyses can be explained by differences in the public policies, social norms or access to healthcare in the places where they live. The large sample matched to death records allows us to introduce county fixed effects, which compare liberals and conservatives within the same counties. This strategy rules out many plausible place-based factors and more cleanly isolates variation between individuals.
As with individual-level characteristics, county-level factors do not fully explain the relationship between ideology and mortality: even conservatives and liberals living in the same county have different health outcomes. These data cast doubt on entirely policy-driven explanations for differences in health outcomes8,24.
Politics and health after COVID-19
By 2020–2022, conservative Americans were less healthy and more likely to die than their liberal peers. Although demographics and place-based characteristics explain some of this gap, a substantial share remains unexplained.
We propose one explanation for this persistent divide: political beliefs increasingly shape consumption of healthcare and thus health outcomes. This notion has been readily applied to COVID-19-related healthcare (for example, vaccines) and outcomes (for example, infection and death rates). But what if those on the political right are less likely to visit, trust and follow the advice of their doctor on health matters entirely unrelated to COVID-19? Existing research shows that while confidence in medicine was once non-partisan, Republicans began to show less confidence than Democrats during the pandemic25,26. At the same time, as liberals have come to trust more in scientific experts, they may have become more compliant with medical advice19. Lower trust and adherence to medical advice correlate with worse health outcomes27, so a broader gap in health could follow.
To measure the relationship between politics and health attitudes and behaviours today, we fielded an original survey that asked respondents a series of questions assessing their willingness to engage with the medical system (N = 21,751). The survey was fielded on an online sample and weighted to approximate national demographics (see ‘Survey methodology’ in Methods for details). A key intervention is analysing not just trust in medicine as an institution, but trust in and behaviours towards individuals’ direct health providers. As it was fielded after the end of the Add Health data, the survey cannot directly test trust as an explanation for changing patterns in health outcomes. Instead, our goal here is to test whether a political gap in trust exists today to motivate future work testing its causal power over time (but see Supplementary Section 10 for suggestive survey evidence on the timing of this gap).
Figure 5 shows the results of regressing measures of engagement with the medical system on respondents’ ideology, partisanship and vote choice (using OLS regression). The models in Fig. 5 include demographic controls and state fixed effects. Supplementary Section 8 presents results from bivariate models and among those respondents that report having chronic diseases (Methods for more details).
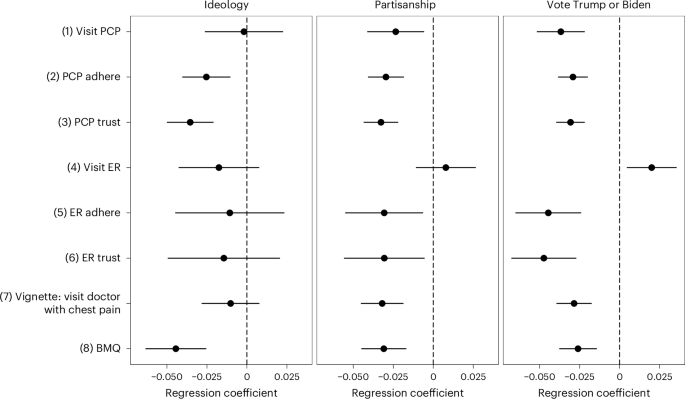
Points represent multivariate OLS regression coefficients of the political variable of interest labelled in the graphical header (covariates specified in Methods); lines represent 95% CIs. Each outcome variable is listed down the left-hand column; rescaled from 0 to 1, where higher values represent that the respondent is more likely to visit, trust and adhere to their PCP or ER physician. Measures of political preference are listed across the top of each model (higher values represent the rightward alternative; partisanship and ideology rescaled from 0 to 1). For example, the first row shows the relationship between visiting one’s PCP and ideology (left), partisanship (middle) and vote choice (right). A total of 16,541 respondents reported supporting either Trump or Biden, 21,694 reported a party identification and 21,722 reported an ideological identification. Full models, statistical reporting and alternative specifications in Supplementary Section 8.
The left-hand plot in Fig. 5 shows the results of regressing measures of engagement with healthcare on self-reported ideology. The other two plots measure health engagement by political beliefs for two political indicators not available in the Add Health data: partisanship (Fig. 5, middle) and Trump–Biden vote choice (Fig. 5, right). We include partisanship and vote choice because they, like ideology, are central to understanding political divisions.
Lines 1–3 in Fig. 5 show the relationship between political beliefs and trust and engagement with one’s primary care provider (PCP). The left-hand plot in Fig. 5 shows no evidence that liberals are more likely than conservatives to have visited their PCP in the prior year (line 1, β = −0.002, 95% CI, (−0.03, 0.02), P = 0.88), but conservatives are significantly less likely to exhibit trust in their PCP (lines 2 and 3, β = −0.035, 95% CI, (−0.05, −0.02), P < 0.001) and follow the advice of their PCP (β = −0.025, 95% CI (−0.04, −0.01), P = 0.001).
The middle and right-hand plots in Fig. 5 show that Republicans and Trump voters are less likely to report having visited their PCP in the past year, and are less likely to trust and follow their advice (lines 1–3; for visit PCP, vote choice (β = −0.037, 95% CI, (−0.05, −0.02), P < 0.001) and partisanship (β = −0.023; 95% CI, (−0.04, −0.01), P = 0.01); for trusting PCP, vote choice (β = −0.031, 95% CI, (−0.04, −0.02), P < 0.001) and partisanship (β = −0.033, 95% CI, (−0.04, −0.02), P < 0.001); for following PCP advice, vote choice (β = −0.029, 95% CI, (−0.04, −0.02), P < 0.001) and partisanship (β = −0.03, 95% CI, (−0.04, −0.02), P < 0.001).
Lines 4–6 in Fig. 5 show the relationship between political beliefs and engagement and trust in an emergency room (ER) doctor, rather than a PCP. Ideology and partisanship are not significantly related to having visited the ER, but Trump voters are more likely to report having been to the ER (β = 0.02, 95% CI, (0.00, 0.04), P = 0.012).
Once at the ER, conservatives and liberals do not exhibit statistically different levels of trust and adherence. However, Republicans are less likely to trust (β = −0.031, 95% CI, (−0.06, −0.01), P = 0.017) and follow the advice of ER doctors than democrats (β = −0.031, 95%CI, (−0.06, −0.01), P = 0.014), and Trump voters are less likely to trust (β = −0.047, 95% CI, (−0.07, −0.03), P < 0.001) and follow advice than Biden voters (β = −0.045, 95% CI, (−0.07, −0.02), P < 0.001).
Line 7 in Fig. 5 examines whether politics predicted people’s willingness to seek care in the case of an emergency. We adopted a vignette from ref. 28, asking respondents how likely they were to go to their primary care doctor if they felt pain in their chest that was so severe that it made them sick, but it wore off in a few minutes. Trump voters and Republicans reported that they would be less likely to go to their primary care doctor if feeling this pain; there is no significant relationship with ideology (vote choice, β = −0.028, 95% CI, (−0.04, −0.02), P < 0.001; partisanship, β = −0.032, 95% CI, (−0.05, −0.02), P < 0.001; ideology, β = −0.01, 95% CI, (−0.03, 0.01), P = 0.27).
Finally, line 8 of Fig. 5, which presents an analysis of only people who report having a chronic illness, shows that vote choice, partisanship and ideology all predict whether a person with a chronic illness is confident in the efficacy of their medications to treat that chronic illness (for example, medicine to treat hypertension) using the Beliefs about Medicines Questionnaire (BMQ; adopted from ref. 29). Right-leaning respondents were more likely to question the usefulness of the medications they use to manage their disease by all 3 measures (vote choice, β = −0.026, 95% CI, (−0.04, −0.01), P < 0.001; partisanship, β = −0.031, 95% CI, (−0.04, −0.02), P < 0.001; ideology, β = −0.044, 95% CI, (−0.06, −0.03), P < 0.001).
Supplementary Section 9 explores the relationship between partisanship, ideology and vote choice, which have become increasingly correlated in recent years. It is unclear why the relationship is weaker by ideology than vote choice or partisanship. One explanation is that about 39% of the sample identifies as neither liberal nor conservative (calling themselves moderate)—a considerably higher rate than the number of people who say they do not align with either party. When looking at trust and engagement by vote choice just among ideological moderates, moderate-Trump and moderate-Biden voters have significantly different health behaviours.
Taken together, these results suggest that right-leaning Americans—as measured by their vote choice, partisanship and to a lesser extent their ideology—are less willing to visit, trust and adhere to the advice of their PCPs. This is true even among people with chronic conditions that require regular contact with the medical system for management and appears across a variety of outcomes unrelated to care for COVID-19.
⚡ **What’s your take?**
Share your thoughts in the comments below!
#️⃣ **#political #polarization #health #outcomes #USA**
🕒 **Posted on**: 1779655457
🌟 **Want more?** Click here for more info! 🌟